The wage war, especially in public safety, is likely not sustainable. A recent study by the National Emergency Number Association (NENA) found that 82% of centers reported being understaffed and struggling with hiring and retention, with respondents citing stress and low pay as the top obstacles to attracting and keeping staff.
This is one reason communities are considering, and DOING, regional consolidation of services.
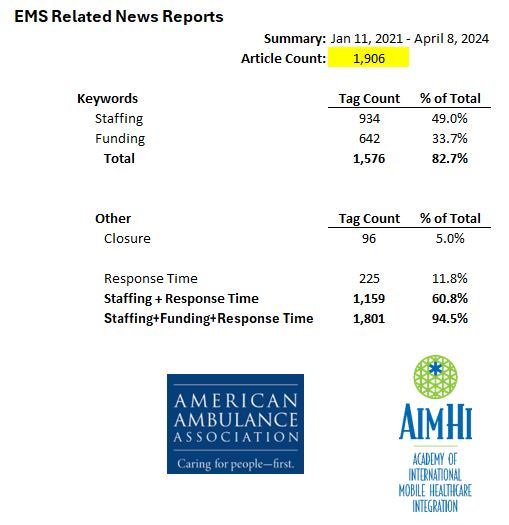
It is also a primary reason for the EMS worker shortage, leading agencies to require funding to raise front-line wages to maintain staffing and service levels.
-----------------
Mounting job vacancies push state and local governments into a wage war for workers
BY DAVID A. LIEB
July 28, 2023
https://apnews.com/article/state-job-vacancies-pay-raises-wage-war-74d1689d573e298be32f3848fcc88f46
FULTON, Mo. (AP) — At the entrance to Missouri prisons, large signs plead for help: “NOW HIRING” ... “GREAT PAY & BENEFITS.”
No experience is necessary. Anyone 18 and older can apply. Long hours are guaranteed.
Though the assertion of “great pay” for prison guards would have seemed dubious in the past, a series of state pay raises prompted by widespread vacancies has finally made a difference. The Missouri Department of Corrections set a record for new applicants last month.
“After we got our raise, we started seeing people come out of the woodwork, people that hadn’t worked in a while,” said Maj. Albin Narvaez, chief of custody at the Fulton Reception and Diagnostic Center, where new prisoners are housed and evaluated.
Public employers across the U.S. have faced similar struggles to fill jobs, leading to one of the largest surges in state government pay raises in 15 years. Many cities, counties and school districts also are hiking wages to try to retain and attract workers amid aggressive competition from private sector employers.
The wage war comes as governments and taxpayers feel the consequences of empty positions.
In Kansas City, Missouri, a shortage of 911 operators doubled the average hold times for people calling in emergencies. In one Florida county, some schoolchildren frequently arrived late as a lack of bus drivers delayed routes. In Arkansas, abused and neglected kids remained longer in foster care because of a caseworker shortage. In various cities and states, vacancies on road crews meant cracks and potholes took longer to fix than many motorists might like.
“A lot of the jobs we’re talking about are hard jobs,” said Leslie Scott Parker, executive director of the National Association of State Personnel Executives.
Lingering vacancies “eventually affects service to the public or response times to needs,” she added.
Workforce shortages worsened across all sorts of jobs due to a wave of retirements and resignations that began during the pandemic. Many businesses, from restaurants to hospitals, responded nimbly with higher wages and incentives to attract employees. But governments by nature are slower to act, requiring pay raises to go through a legislative process that can take months to complete — and then can take months more to kick in.
Meanwhile, vacancies mounted.
In Georgia, state employee turnover hit a high of 25% in 2022. Thousands of workers left the Department of Corrections, pushing its vacancy rate to around 50%. The state began a series of pay raises. This year, all state employees and teachers got at least a $2,000 raise, with corrections officers getting $4,000 and state troopers $6,000.
The Georgia Department of Corrections used an ad agency to bolster recruitment and held an average of 125 job fairs a month. It’s starting to pay off. In the first week of July, the department received 318 correctional officer applications — nearly double the weekly norm, said department Public Affairs Director Joan Heath.
Almost 1 in 4 positions — more than 2,500 jobs -- were empty in the Missouri Department of Corrections late last year, which was twice the pre-pandemic vacancy rate in 2019.
Missouri gave state workers a 7.5% pay raise in 2022. This spring, Gov. Mike Parson signed an emergency spending bill with an additional 8.7% raise, plus an extra $2 an hour for people working evening and night shifts at prisons, mental health facilities and other institutions. The vacancy rate for entry level corrections officers now is declining, and the average number of applications for all state positions is up 18% since the start of last year.
At the Fulton prison, where staff shortages have led to a standard 52-hour work week, newly hired employees can earn around $60,000 annually — an amount roughly equal to the state’s median household income. The prison also is proposing to provide free childcare to correctional officers willing to work nights.
If prison staffing is too low, “it can get dangerous” for both inmates and guards, Narvaez said.
Public safety concerns also have arisen in Kansas City, where a country music fan attacked before a concert last month waited four minutes for a 911 call to be answered and an hour for an ambulance [from Kansas City Fire Department] to arrive. About one-quarter of 911 call center positions are vacant — “a huge factor” in the longer wait times to answer calls, said Tamara Bazzle, assistant manager of the communications unit for the Kansas City Police Department.
In Biddeford, Maine, a 15-person roster of 911 dispatchers dipped to just eight employees in July as people quit a “pressure cooker job” for less stress or better pay elsewhere, Police Chief JoAnne Fisk said. The city is now offering fully certified dispatchers $41 an hour to help plug the gaps on a part-time basis — $10 an hour more than comparable new workers normally would earn.
This month, Biddeford also launched a $2,000 bonus for city employees who refer others who get jobs. That comes a year after Biddeford adopted a four-day work week with paid lunch periods to try to make jobs more appealing, said City Manager Jim Bennett.
To attract workers, other governments have dropped college degree requirements and spiced up drab job descriptions.
Nationally, the turnover rate in state and local governments is twice the average of the previous two decades, according to federal labor statistics.
Uncompetitive wages were the most common reason for leaving cited in exit interviews, according to a survey of 249 state and local government human resource managers conducted by MissionSquare Research Institute, a Washington, D.C. -based nonprofit. The hardest positions to fill included police and corrections officers, doctors, nurses, engineers and jobs requiring commercial driver’s licenses.
Along Florida’s east coast, the Brevard County transit system and school district have been competing for bus drivers. On days when drivers are lacking, the transit system has cut the frequency of bus stops on some routes. The school system, meanwhile, has asked some bus drivers to run a second route after dropping children off at school, often resulting in the second busload arriving late.
Since 2022, the county has twice raised bus driver wages to a current rate of $17.47 an hour. The school board recently countered with a $5 increase to a minimum $20 an hour for the upcoming school year. The goal is to hire enough drivers to regularly get kids to class on time, said school system communications director Russell Bruhn.
In Arkansas, the goal is to get foster kids into permanent homes in less than a year. But during the first three months of this year, the state met that target for just 32% of foster children — well below the national standard of over 40%. More than one-fifth of the roughly 1,400 positions in the Arkansas Division of Children and Family Services are vacant.
Many new employees leave in less than two years because of heavy caseloads and the “very difficult, emotionally tolling work,” Mischa Martin, the Department of Human Services’ deputy secretary of youth and families, told lawmakers last month.
“If we had a knowledgeable, experienced workforce,” she said, “they would be able to work cases in a better way to get kids home quicker.”